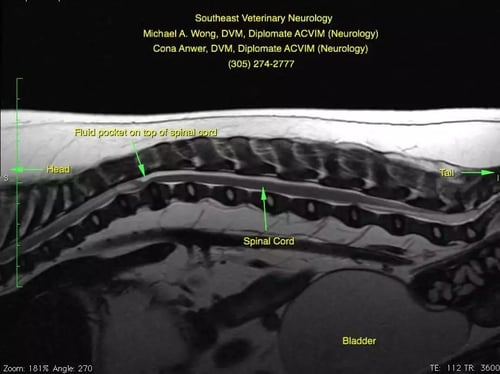
Wellington's MRI
Wellington has a fluid buildup dorsal to the spinal cord that is compressing the spinal cord ventrally. Additionally, cranial to the dorsal buildup of cerebrospinal fluid (CSF), you can see that there is increased signal (“brightness”) within the spinal cord. This is the ‘classic’ finding of a relatively newly recognized disease. There are several different names that neurologists have used for this disease including “Pug Myelopathy”, “Pug Constrictive Myelopathy”, “facet hypoplasia”, “subarachnoid diverticulum” and others. Although little is published about this condition, in my experience, it is the most common cause of mid-back spinal cord problems in Pugs.

Wellington's Surgery
Since so little is known about the condition, there is no consensus among neurologists about the best way to treat it. My (Dr. Wong) experience has been that early surgical intervention carries the best chances of helping. Surgery is challenging, in that it involves a hemi- or dorsal laminectomy, durotomy/durectomy, gentle breakdown of the constriction and stabilization of the spine.
Dr. Wong is using an operating microscope which aids in lighting and magnification which is essential when performing this particular surgery (e.g. durotomy/durectomy and removing the ‘scar tissue’ from the subarachnoid space. The operating microscope is located in the upper left of the screen. The viewing screen in the upper right of the photo is similar (lower resolution) to what Dr. Wong sees through the microscope. In the viewer, cranial is to the left of the viewing screen and caudal is to the right. You are looking at the vertebral column. Two screws have been placed caudally and a third screw is being placed. Wellington is at the bottom of the screen, where you can see Dr. Wong’s hands and the drill.
Post-operatively, radiographs are performed to confirm accurate placement of the implants.
Many dogs with subarachnoid diverticula (Pug constrictive myelopathy/facet hypoplasia) do very well with surgery. Relapses are possible, but in my experience, they typically happen 2-3 years later. Unfortunately, not enough is known to make strong recommendations.