Luna Bell’s examination indicates a neurological problem affecting the C1-C5 spinal cord. She is alert and responsive, has normal cranial nerves, has postural reaction deficits in all four limbs, but has normal spinal reflexes in all four limbs.
Possible causes include a malformation such as atlantoaxial instability, Chiari-like malformation and syringomyelia, meningitis/myelitis, infection, slipped disc (unlikely based on age), tumor (unlikely based on age) or other less likely cause.
Radiographs of the cervical vertebral column were performed.
There is increased space between the dorsal aspect of C1 and the cranial/dorsal aspect of C2. There is subluxation at C2 relative to C1, with dorsal angulation of the caudal portion. Note that one cannot visualize the spinal cord nor the intervertebral discs. Additionally, there is an overlap of structures within the cervical region. Atlantoaxial instability and subluxation was diagnosed through the radiographs.
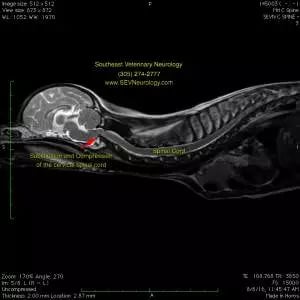
An MRI was performed to further define the abnormalities. Multiple congenital abnormalities can occur concurrently (e.g. synovial cyst associated with AA instability, etc). MRI shows these soft tissue abnormalities best and is the only way to diagnose Chiari-like malformation and syringomyelia.
MRI is superior for evaluating the soft tissues of the brain, spinal cord, meninges, and discs. Note the ‘kinking’ of the cranial cervical spinal cord where it is being compressed by the dorsal subluxation of C2 relative to C1.
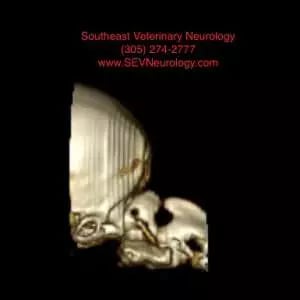
At Southeast Veterinary Neurology, we typically perform a CT scan prior to surgery. While MRI is the ideal way of imaging the spinal cord and brain, CT is excellent for evaluating the bone. The treatment of choice for atlantoaxial instability is surgical stabilization with screws and bone cement. Since AA instability is typically diagnosed in small dogs (sometimes less than 1kg), pre-operative planning for size and angle of the implants is indicated. Below is a 3-dimension reconstruction of Luna Bell’s cervical vertebral column and caudal skull. CT and MRI are able to be performed under the same anesthetic period at Southeast Veterinary Neurology.
At Southeast Veterinary Neurology, we have the ability to print 3D images of our CTs. Below is a 3D print of Luna Bell’s vertebral column. This can be used to help plan the surgery.